- Joined
- Oct 7, 2008
- Messages
- 64,196
- Location
- Bulgaria
Suicide by hanging.

Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.

That doesn't make any sense. Clearly something else going on in his mind. The whole point of avoiding untrustworthy vaccinations is to preserve your life, not so that you can die in a much more dramatic fashion instead.Dramatic Suicide of an Anti-Vax Man in Italy









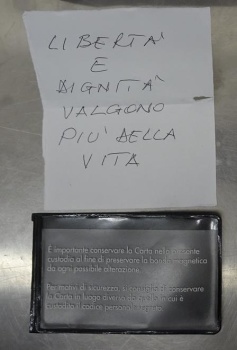
In January 2022 a 58-year-old man jumped under a train in Italy. A suicide note was found in his pocket along with several tablets of Xanax. The suicide note read "Freedom and Dignity Are Worth More than Life." Relatives later told police the man was strongly against covid vaccines and restrictions. Investigaion concluded that the train was going at more than 150 km/h at the time ripping and shredding the man on impact.











That sucks. Poor guy.
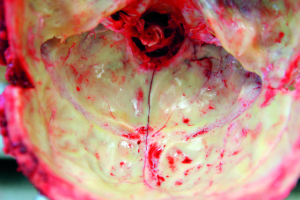
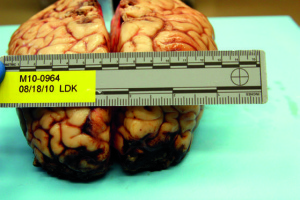
Forensic autopsy case of a 54-year-old male who was found in a forest in late November, approximately 500 m away from his car.
He was positioned bent over a trunk of a tree with his head beneath the rest of his body. His pants were down to his knees, and there were soiled blades of grass and leaves on his body. Investigation of the case circumstances revealed that he had attempted suicide by carbon monoxide poisoning, using a hose connected to the exhaust pipe and running it through the window into the cabin. Window on the driver’s side was broken with glass particles on the driver's seat. Wrappers from “Rivotril” tablets, a generic benzodiazepine, were also found in the car.
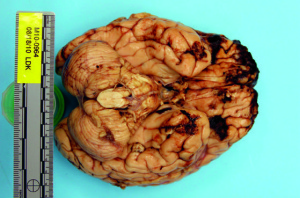
Autopsy revealed the following: postmortem hypostasis was of a cherry red color and well pronounced on the upper part of the front of the body and face. Numerous bruises, contusions, and erosions were present all over the body. Frostbites were especially pronounced in the knees and elbows area. The synovial membranes were partially bloodstained and reddish in color. Opening the stomach revealed erosions of the gastric mucosa (Wischnewsky sign).
Chemical toxicological analysis detected presence of benzodiazepines and carboxyhemoglobin (25%).
Conclusion
Based on the autopsy findings, chemical toxicological analyses, and investigation of the case circumstances, it has been concluded that the death occurred due to the combined effects of hypothermia, postural asphyxia and carboxyhemoglobin and benzodiazepine intoxication. The manner of death in this case is a combination of accidental and suicidal, as the victim attempted suicide but ultimately died due to exposure to low external temperature.
He shot him self necked. He must have known the dogs were gonna eat him. Why else would he do that? I wonder if he rubbed food to those areas of his body to entice the dogs.Cat and dog scavenging at indoor forensic scenes
A 53-year-old man was found dead on the floor in his flat in December. His unclothed body was partially mummified. The PMI was estimated to be long, about 2–3 weeks due to decomposition. An entry gunshot wound was present in his right forehead, an exit wound was not found and no CT imaging was performed. Soft tissue is missing from the right side of the skull, the right arm, the lower abdomen and genital region; the right pelvic area, the right leg and the bones are partially exposed. The skin margins are frayed and irregular; the skin surface near the margins is intact. The arm bones are missing from the distal right humerus downwards and the leg bones from the distal right femur downwards, an approx. 20-cm-long shaft fragment of the right fibula was found nearby the body. The distal femur bone end was irregularly fractured with pits near the fracture line. The distal end of the fibula shaft showed a spiral fracture. Especially in the area of the pelvis and the right upper thigh, the mummified tendon and ligament remains are preserved as frayed fibres. The cause and manner of death was a suicidal gunshot to the head; no autopsy was performed. There were three large dogs in the flat, two Belgian and a German shepherd.
I've known several people who took their own lives. Two of them literally starved themselves to death out of depression, and one came close to it. Another one I don't know why except that he just didn't seem to gel with his parents at all and hung himself at 16, another one had unresolved mental health problems while at school and died age 25, another one had problems with his penis but I also discovered afterwards had problems with acceptance from his parents over his sexuality, and hung himself when he was about 50. One of the ones who starved himself to death nearly killed himself 20 years earlier, and the other one who starved herself to death I spoke to only the day before she died trying to urge her to have some therapy. Another one killed himself in a way I don't know, but he was bipolar and seemingly more depressed most of the time. His boyfriend then killed himself in a very planned, relatively neat and organised way to make it easy for people (in the bath, but water running to wash the blood away, timed email delivery). Another one's life and physical health had been reduced to a shadow of what it had been and he hung himself, which I had sort of been expecting but could do nothing to help his situation. What I can tell you is that most people who take their own lives are rarely in a state of mind where they have the mental resources to consider ongoing consequences however obvious they may seem to us; they are in unbearable distress from which there doesn't appear to be any escape in this life and they just want it to end.He shot him self necked. He must have known the dogs were gonna eat him. Why else would he do that? I wonder if he rubbed food to those areas of his body to entice the dogs.
Thanks for the response. You make valid points. You sure know a-lot of people who killed themselves. Not trying to be facetious, but seriously you know a-lot. I always wish i could save people that are gonna off themselves.I've known several people who took their own lives. Two of them literally starved themselves to death out of depression, and one came close to it. Another one I don't know why except that he just didn't seem to gel with his parents at all and hung himself at 16, another one had unresolved mental health problems while at school and died age 25, another one had problems with his penis but I also discovered afterwards had problems with acceptance from his parents over his sexuality, and hung himself when he was about 50. One of the ones who starved himself to death nearly killed himself 20 years earlier, and the other one who starved herself to death I spoke to only the day before she died trying to urge her to have some therapy. Another one killed himself in a way I don't know, but he was bipolar and seemingly more depressed most of the time. His boyfriend then killed himself in a very planned, relatively neat and organised way to make it easy for people (in the bath, but water running to wash the blood away, timed email delivery). Another one's life and physical health had been reduced to a shadow of what it had been and he hung himself, which I had sort of been expecting but could do nothing to help his situation. What I can tell you is that most people who take their own lives are rarely in a state of mind where they have the mental resources to consider ongoing consequences however obvious they may seem to us; they are in unbearable distress from which there doesn't appear to be any escape in this life and they just want it to end.
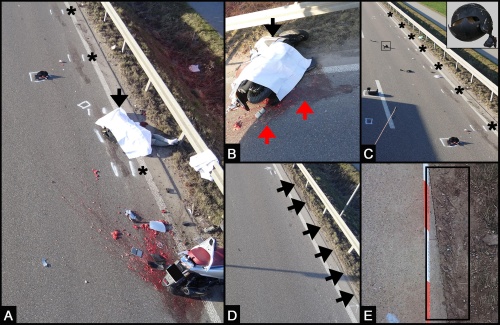
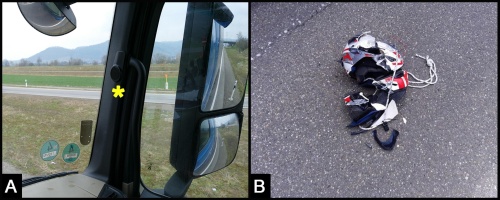
That sucks.69-year-old motorcyclist was run over by a truck on a highway in Germany.
It's really tragic. Most died before I realised they were headed that way, except the guy whose quality of life and circumstances had deteriorated in ways and circumstances I could do nothing about during lockdown. But I did get suicidal worker support for him, it just wasn't enough.Thanks for the response. You make valid points. You sure know a-lot of people who killed themselves. Not trying to be facetious, but seriously you know a-lot. I always wish i could save people that are gonna off themselves.
To give a bit more detail, and I think this is probably one of the few places I won't get flamed for saying these things, a significant number of them I came into contact with because I was running a support group for people diagnosed HIV+ - but not from a conventional perspective, these were all people who were either challenging the treatment they'd been prescribed or questioning their diagnoses - for good reason. HIV / AIDS science is a total shit-show. There are three versions of reality: What most people think happened, what actually happened, and what should have happened. And the problems are all the way from molecular biology to epidemiology, taking in biology, virology and pharmacology along the way, to name a few. In case you're not aware, there are around 90 other things already documented in medical literature that can make HIV tests that are used to diagnose you positive. That's because the proteins and antibodies that are supposed to be specific to HIV are anything but specific. For example, there are around 7 studies (from memory) that show Hep B vaccination can trigger false positives for a period of time afterwards, with the peak at about 3 months after the vaccination. Also, flu, swine flu, tetanus among others. But woe betide you if you get diagnosed during that window period after vaccination - you've got the diagnosis for life. And don't think viral load tests or phylogenetics will save you: No actual HIV test of any type has ever been correlated with actual HIV in the body. There is no electron microscopy of HIV in anyone's blood published anywhere. What you see is pictures of culture. But it was already known that stressing cells can make them rearrange their own DNA and create particles. In 2016 a paper was published where a team including Robert Gallo actually admitted that the particles stressed cells put out may be neutral or even beneficial. And they also admitted that they can't tell them apart from what they believe to be HIV particles. That is not all there is, that is just ONE loose thread dangling. In one criminal case I was involved in, we did electon microscopy of the defendant's blood - significant viral load, but no visible particles even vaguely resembling HIV in his actual blood, from the same blood sample.Thanks for the response. You make valid points. You sure know a-lot of people who killed themselves. Not trying to be facetious, but seriously you know a-lot. I always wish i could save people that are gonna off themselves.
Hi @baddog007 i want to take more time to digest and respond when i free up this week.It's really tragic. Most died before I realised they were headed that way, except the guy whose quality of life and circumstances had deteriorated in ways and circumstances I could do nothing about during lockdown. But I did get suicidal worker support for him, it just wasn't enough.
The girl who starved herself to death had been abused by her father for years and her mother had done nothing to stop it. She had crushingly low self-esteem. I repeatedly told her that she was stiff the wrong type of therapist (cognitive behavioural therapy) which is next to useless for dealing with historical roots of a problem, but she was getting the therapy for free on the NHS and didn't make it a priority to save up for the type is therapy I recommended (NLP and time line therapy) which has tools specifically for dealing with historical events. Eventually she had a mental breakdown and was taken to hospital, but after recovering just stopped eating. She had lost the appetite for life. The tragedy of poor quality therapy is that she then rejected all therapy, but effective therapy is like finding the combination of the lock after years is trying the wrong numbers.
To give a bit more detail, and I think this is probably one of the few places I won't get flamed for saying these things, a significant number of them I came into contact with because I was running a support group for people diagnosed HIV+ - but not from a conventional perspective, these were all people who were either challenging the treatment they'd been prescribed or questioning their diagnoses - for good reason. HIV / AIDS science is a total shit-show. There are three versions of reality: What most people think happened, what actually happened, and what should have happened. And the problems are all the way from molecular biology to epidemiology, taking in biology, virology and pharmacology along the way, to name a few. In case you're not aware, there are around 90 other things already documented in medical literature that can make HIV tests that are used to diagnose you positive. That's because the proteins and antibodies that are supposed to be specific to HIV are anything but specific. For example, there are around 7 studies (from memory) that show Hep B vaccination can trigger false positives for a period of time afterwards, with the peak at about 3 months after the vaccination. Also, flu, swine flu, tetanus among others. But woe betide you if you get diagnosed during that window period after vaccination - you've got the diagnosis for life. And don't think viral load tests or phylogenetics will save you: No actual HIV test of any type has ever been correlated with actual HIV in the body. There is no electron microscopy of HIV in anyone's blood published anywhere. What you see is pictures of culture. But it was already known that stressing cells can make them rearrange their own DNA and create particles. In 2016 a paper was published where a team including Robert Gallo actually admitted that the particles stressed cells put out may be neutral or even beneficial. And they also admitted that they can't tell them apart from what they believe to be HIV particles. That is not all there is, that is just ONE loose thread dangling. In one criminal case I was involved in, we did electon microscopy of the defendant's blood - significant viral load, but no visible particles even vaguely resembling HIV in his actual blood, from the same blood sample.
So anyway, the science is totally shit. What HIV tests represent really is a range of stressors on the human body. In Africa this can be Malaria or other parasitic infections which has already been acknowledged by a team that included someone from the Health Protection Agency in the UK. However, from my couple of decades on the front line of supporting people questioning things and involvement in multiple legal cases behind the scenes, a picture began to emerge that there was typically something different about people diagnosed HIV+: they tended to have 'issues'. They tended to be more fragile for one reason or another. A German doctor first crystalised my thoughts when she said, "I couldn't help noticing that my HIV patients were more vulnerable to the world". I've now refined that and the first thing I ask now is, "Have you been under any serious stress in the last few years?". Usually the answer is yes. Typically it will be a high level of stress, about something existential, from which there doesn't appear to be any escape or against which you can't fight back. Some people have been damaged by some kind of abuse in their past that they haven't resolved. Some people have just found themselves in unusual and highly stressful circumstances. For example, one girl had made a £1m from online businesses, and gave it to someone she trusted to invest, and he lost the whole lot. It really destabilised her for a while, and afterwards, when she got pregnant, she was HIV+. She got all four guys who were the only ones she could ever have caught it from tested, and they were all negative - this is quite a common experience, by the way, if there is a limited number of people someone could conceivably have caught something from, to find that the only people you could have caught something from are all negative, but doctors go into denial about it.
Even a boyfriend of mine when I was in a relationship with him when he was diagnosed, had had a very traumatic upbringing, and was still tortured at the time as to whether he was going to heaven or hell for being gay - that's existential stress of the highest order. So when he was persuaded to get tested and was HIV+, it meant punishment from God to him. Luckily, I quickly re-read most of the science I'd already been reading, just to check I hadn't been wrong, and it was just overwhelmingly obviously a scientific fuck-up. So I told him we'd carry on having sex the way we were, which was unprotected, no PrEP, no ARVs, and him ejaculating inside me all the time. Nope, I never caught anything in the rest of that relationship. And part of the reason for him being diagnosed HIV+ I came to realise also was because black people are much more susceptible to false positives, according to not only statistics, but Dr Rodney Richards, one of the designers of the original Abbot Laboratories HIV tests. That's because people with sub-saharan heritage have a much stronger antibody response by about 40%, so it's much easier to hit the arbitrary threshold that is called 'HIV+' And he'd recently had a Hepatitis B vaccination when he was tested.
So anyway, that's why I got into being an activist in that area, and that's how I came to know a lot of people who were psychologically vulnerable, and as a result, much more likely to be diagnosed HIV+. That doesn't account for all of them. The 16yo I just don't know why as I hadn't seen him for 5 years, it was our mums who kept in touch. The 25yo had mental problems anyway and I hadn't seen him for years. The guy whose life and health had fallen apart was a refugee I'd helped to get granted asylum, but he'd had a stroke from high blood pressure and his circumstances were just really bad. Everyone else had been diagnosed HIV+. But it wasn't 'AIDS' that got them, it was their other shit that eventually they couldn't handle for one reason or another.